What is the best protocol for endometrial preparation for vitrified donor oocyte thaw?
From 1/1/22 through 4/15/25 our center has performed 88 single day 5 fresh embryo transfers after vitrified donor oocyte thaw and ICSI. We have patients start oral estradiol 2mg three times a day on menses cycle day 1-3 and then do transvaginal ultrasound and check estradiol and progesterone on cycle day 12 to 16. Most commonly we see patients on cycle day 12.
We aim for a trilaminar endometrium with thickness of 7.0mm or greater. If the endometrium is thin we typically add vaginal estradiol 2mg daily and see them back in 4-7 days for a repeat lining check. Once the lining is appropriate we start progesterone in 1 to 4 days and transfer on the 6th day of progesterone. We typically thaw oocytes in the morning and then start progesterone the same day in the evening. We use Prometrium 200mg vaginally 3 times a day (TID) or Endometrin 100mg vaginally TID. For patients also taking progesterone in oil (PIO) we add 50mg PIO IM every 3 days. We use Endometrin approximately 25% of the time and Prometrium 75% of the time. We see no differences between Endometrin and Prometrium.
We define an ongoing pregnancy as a fetal heartbeat detected at or after 8 weeks 0 days gestation and no report to our clinic of a spontaneous abortion by 14 weeks 0 days gestation.
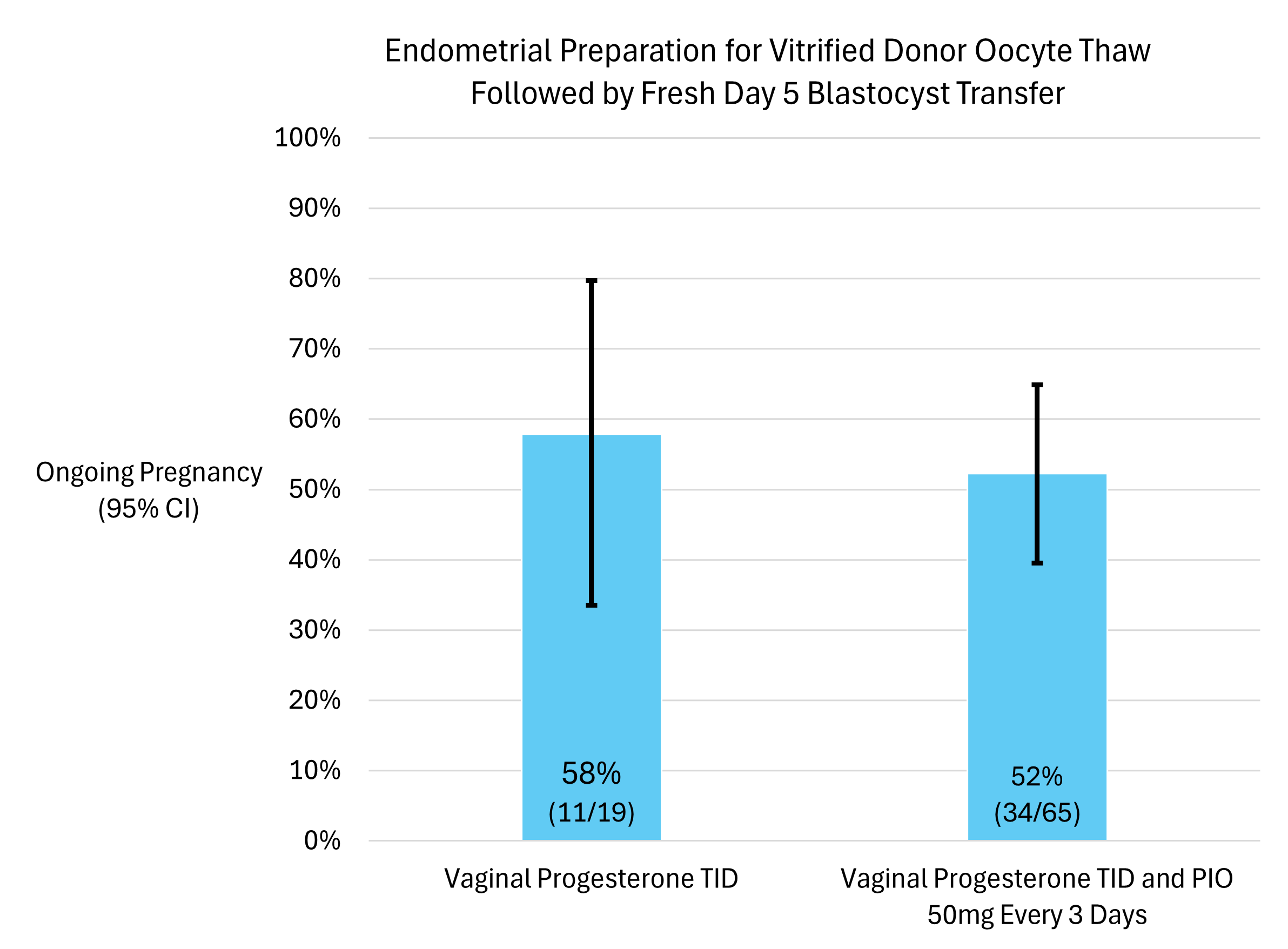
Our most common protocol is Vaginal Progesterone TID and PIO 50mg IM Every 3 days which resulted in an ongoing pregnancy rate of 52% per single embryo transfer.
Our next most common protocol was Vaginal Progesterone TID which resulted in an ongoing pregnancy rate of 58% per single embryo transfer.
We had 1 transfer after modified natural cycle (Ovidrel trigger and vaginal Prometrium 200mg daily starting 4 days after trigger with oocyte thaw 36 hours after Ovidrel trigger) which resulted in an ongoing pregnancy. Another was a modified natural cycle with the addition of FSH which resulted in ongoing pregnancy. Another one was modified natural with addition of letrozole 5mg PO cycle days 3-7 and this resulted in ongoing pregnancy. One cycle used PIO 100mg IM daily and this resulted in ongoing pregnancy. In general our lab has a preference against natural cycles for donor oocyte thaw embryo transfers due to challenges with staffing.
It is challenging to study laser assisted hatching (LAH) since our embryologists prefer not to do LAH when the embryo is expanding and the zona pellucida is thinning. Therefore sometimes LAH is ordered but not performed if the zona is thinning. We do not do LAH 56% of the time, we do use LAH 27% of the time, and 17% of the time LAH is ordered but not performed due to zona pellucida thinning. We do not see any differences in ongoing pregnancy associated with whether or not LAH was performed.
This research has been approved by the Christ Hospital IRB (protocol #25-030).